
VBAC After Cesarean for Arrest of Descent or CPD
VBAC after Cesarean for Arrest of Descent or Cephalo-Pelvic Disproportion – written by Pamela Vireday
 |
A cesarean for “Arrest of Descent” means a cesarean done after a woman has dilated fully and pushed for a while without the baby descending. The amount of pushing time required for the diagnosis varies from source to source but is usually at least 1-3 hours.
When a woman has a cesarean for Arrest of Descent, she is often told something is wrong with her pelvis. She might be told she has:
- A “flat” sacrum
- A “prominent” sacrum
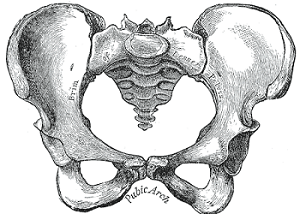
- A pubic arch that is “too narrow”
- Ischial spines that are “too prominent”
- A pelvis that is “too small”
- “Too much soft tissue” (fat) lining the vagina/pelvis
- A pelvis that is the “wrong shape”
- A baby that was “too big” for her pelvis
- “Cephalo-Pelvic Disproportion” (baby too big and pelvis too small, causing baby to not fit)
Often women who have been told these things are strongly discouraged from tryingfor a Vaginal Birth After Cesarean (VBAC). There are documented cases where women have been told their pelvis is too flat or too small to have a VBAC, that they have “soft tissue dystocia” (a.k.a. “fat vagina“), that their pelvis is the wrong shape, or that since they couldn’t push out a baby before, chances are they never will be able to because CPD is a recurring condition:
Yesterday, at my appt, while speaking with one of the midwives – she asked if I wanted her honest opinion & that if I was unable to push out a 7 and 1/2 pound baby and 2nd babies are normally larger then she didn’t think it would be successful.
The bottom line is that providers that are not truly VBAC-supportive often make women believe that something is wrong with their bodies and that they have little chance of having a vaginal birth, implying it’s better just to schedule a repeat cesarean. Then the care providers conveniently have fewer VBAC labors to attend.
However, many women who have been told they have an abnormal pelvis or soft tissue dystocia or who have had a cesarean for Arrest of Descent or CPD have gone on to have VBACs anyhow.
And a new study just out confirms that many women with a prior cesarean for Arrest of Descent do indeed go on to have a VBAC and should not be discouraged from trying.
New Study on VBAC after Arrest of Descent
A recent American study (Fox 2018) shows that VBAC after prior Arrest of Descent is often successful.
In the study, one hundred women who had one prior cesarean for Arrest of Descent had a “Trial Of Labor After Cesarean” (TOLAC or TOL). A whopping 84% ended up having a VBAC. This is an excellent rate and better on average than many VBAC studies.
The authors concluded (my emphasis):
This suggests that arrest of descent is mostly dependent on factors unique to each pregnancy and not due to an inadequate pelvis or recurring conditions. Women with a prior CD [Cesarean Delivery] for arrest of descent should not be discouraged from attempting TOLAC in a subsequent pregnancy due to concerns about the likelihood of success.
The fact that the authors state this so strongly in an obstetrics journal is a big deal because it goes against what is commonly taught to many OBs, so let’s reemphasize those points:
- Arrest of Descent is NOT usually due to an inadequate pelvis
- “CPD” is not necessarily a recurring condition
- Women with this history should not be discouraged from trying for a VBAC
Other Similar Studies
Was this study just a fluke? What do other studies on Arrest of Descent say?
There are only a couple of studies that specifically use the term “VBAC after Arrest of Descent” so you have widen the search a bit. Other search terms to consider include “CPD + cesarean,” “cesareans after full dilation,” or “cesareans done during second stage of labor” (pushing), or “prolonged second stage,” or similar terms. Carefully vetted, these are essentially Arrest of Descent cesareans too.
If you just look at studies that examine VBAC after a cesarean for CPD, research reviews show that about two-thirds of women will have a VBAC. This rate is lower than for those whose first cesarean was for breech or fetal distress, but is still a very good rate. If all those women had been discouraged from VBAC or pressured into repeat cesareans, two-thirds of them would have had unnecessary cesareans!
There is very little data on women who have had more than one cesarean for CPD. However, one 1989 study did contain some data on women like this. If you crunch the data in the full text of the study, women with 2 prior cesareans for CPD had a 56% VBAC rate. So although we don’t have a lot of data on this, what we do have suggests that even among women with more than one cesarean for CPD, more than half will have a VBAC.
The doctors who like to discourage VBAC cite a discouraging 1997 study that found a low VBAC rate (13%) in women who had reached full dilation and pushed in their previous labor. However, the rest of the research is much more encouraging.
In one Californian study from 2015, 54% of women with no prior vaginal birth and a prior cesarean during pushing stage went on to have a VBAC. In other words, they were just as likely to have a VBAC as not.
Similarly, a Danish study found a 59% VBAC rate in women whose cesareans occurred at 9-10 cm of dilation (9 cm often represents a fully dilated woman with a cervical lip, likely due to fetal malposition). Again, more than half had a VBAC and avoided the risks of additional surgery.
But some studies have results even better than that. In a New York study, 74.5% of women with prior pushing-stage cesareans went on to have a VBAC, some of them with forceps help, which suggests that fetal malpositions were an issue for quite a few.
Echoing those numbers is a Canadian study that found a 75% VBAC rate in those with a prior second stage dystocia cesarean. A very small, older Irish study found a 73% VBAC rate in those with a prior cesarean in the second stage.
Similarly, an older Dutch study found an 80% VBAC rate in those with a prior Arrest of Descent cesarean. This echoes our current Fox 2018 study that found an 84% VBAC rate after prior Arrest of Descent.
In summary, the majority of the research clearly supports the idea that women with a prior cesarean that occurred after full dilation and pushing can be offered a “trial of labor after cesarean” and will have a quite reasonable chance for a VBAC.
In the end, the decision whether to go for a VBAC is the mother’s, but she should be reassured that she is just as likely to have a VBAC as not, and in many practices, especially with proactive care regarding fetal position, her chances are even better.
The Importance of Fetal Position
So what causes Arrest of Descent? Why does it happen in some births but not others in the same mother? The answer is usually fetal position.
In Arrest of Descent/CPD cesareans, the problem is usually the BABY’S POSITION, not the mother’s pelvis.
If the baby is not well-positioned, labor tends to be slow and extra painful. It often slows or stalls between 4-7 cm of dilation. Often the mother eventually dilates fully but there is little or no progress during pushing. Fetal distress may occur.
Some providers become impatient and intervene with procedures (like breaking the waters) which may do more harm than good. Frequently, they are too quick to move to surgery when more patience might see the position resolve or the baby be born just fine in the “less-optimal” position. Recent research suggests that more than three-fourths of women with prolonged pushing stages (more than 3 hours) will deliver vaginally if just given a little more time.
What kind of fetal positions can cause problems? Read here for illustrations and specifics of the different fetal positions. The Spinning Babies website also has many helpful articles and illustrations on fetal position and how to help create maximum room in the pelvis. In the meantime, below is a brief introduction of the most common fetal malpositions.
Keep in mind that Presentation refers to which part of the baby is presenting first, and Position refers to how the baby is oriented in the mother’s body in a head-down position. Also keep in mind that when describing fetal position, obstetric texts reference the back of the baby’s head (the occiput) and which way the occiput is oriented in relationship to the mother. Most laypeople find it easier to understand by thinking of which way the baby is looking, so I use both in my descriptions.
Both the Spinning Babies website and The Labor Progress Handbook by Penny Simkin et al. have many ideas for various ways to help malpositioned babies resolve their position, and for creating more space in the pelvis. We will discuss this further in future posts.
 |
| Occiput Anterior or OA |
The easiest fetal position for labor and birth is usually Occiput Anterior. This is abbreviated OA and means the baby is head-down with the back of the baby’s head against the mother’s front; in other words, the baby is looking towards the mother’s back. This position is considered the norm and the vast majority of babies will be born in this position.
Direct OA is when the baby is looking directly back at the mother’s sacrum. LOA is when the baby is mostly facing the mother’s back but his back is a bit towards the left side; ROA is the same but a bit towards the right side.
Ideally, the baby’s chin is tipped towards its chest so the smallest possible diameter of its head presents. If the baby’s head is not well-flexed, the presenting diameter is a bit larger. If the baby’s head is tipped to one side or the other, it can be even larger. More on that below.
Occiput Posterior
 |
| Illustration by Gail Tully, Spinning Babies |
One of the most common fetal positions that can cause problems during labor is the Occiput Posterior position. This is abbreviated OP; the back of baby’s head is against your back and baby is looking at your tummy. If the baby is directly facing your back, that’s direct OP; if it’s a little to the right or left, then that’s ROP or LOP.
Although many babies enter labor in less-ideal positions like OP, only about 5% stay posterior all through labor and deliver that way. Babies that come out in the OP position are sometimes called “Stargazers” or “Sunny Side Up.”
By itself, an OP position does not have to mean a cesarean, since most OP babies turn during labor and become OA before birth. The labor may be a little longer and more painful but it often proceeds just fine with a little patience. However, babies that are persistently posterior all the way through labor and birth have a high rate of problems.
Research clearly shows that persistent posterior babies have higher rates of cesareans for CPD or Arrest of Descent. This is because the presenting head diameter of a baby in OP position is larger than the baby in an OA position. In addition, the back of the baby’s head is against the mother’s back and that makes for a more painful labor, with lots of back labor and a slower dilation. This in turn often means lots of interventions from care providers that may make the situation worse, like breaking the waters, which takes away the cushion for baby to turn more easily and may lead to fetal distress.
However, OP babies do not always end with cesareans. With time and patience, an OP baby with a flexed head (chin to chest) can often be born vaginally. Alternatively, a vaginal birth may be possible if the care provider is patient and allows extra time for the baby’s head to mold enough to descend into the pelvis. When it hits the pelvic floor, it often then rotates from OP to OA on the perineum and may be born quickly. Often an OP baby can be helped to rotate to OA through manual rotation, an instrumental delivery, or maternal postural changes like the all-fours position.
But because of the impatience of many providers, the fetal distress that can occur, and the extra-painful, longer labors associated with OP babies, many persistent OP babies end up being born by cesarean.
Deflexed Heads

If a baby’s head is deflexed (not chin to chest), this can cause problems as well. A deflexed head makes the baby’s presenting head diameter larger. This means the baby may not fit through very well, or the baby needs extra time for its head to mold enough to get through. OA babies with mildly deflexed heads experience longer labors, but with a little patience, are usually able to be born vaginally.
However, significant problems can occur if deflexion is extreme. Extreme examples of deflexed heads include a brow (forehead first) or face (face-first) presentation. Although vaginal births of brow and face presentations have been documented, most often they end in cesarean these days unless the baby’s position can be resolved. Fortunately, brow and face presentations are quite rare.
Deflexed babies in an OP position are fairly common and result in many long, difficult labors. OP babies already start out with a larger presenting head diameter; when they also have deflexed heads (known as a “military” position), this makes the head diameter even larger. Big OP babies often have deflexed heads, making their head diameters even larger. These babies often have extremely long and hard labors, and many end in cesareans. Turn the baby around and/or tip its chin towards its chest so that the head is flexed and the baby would likely fit much better; many cesareans could be avoided.
Occiput Transverse/Transverse Arrest
| Occiput Transverse, which can result in Transverse Arrest |
When a baby’s head is directly sideways, facing the hip, this is called Occiput Transverse or OT. Often OT positions are able to resolve to OA, but sometimes they do not and result in a vacuum extraction, forceps delivery, or cesarean.
OT often occurs when the baby was posterior earlier in labor, tries to rotate to anterior, and gets stuck in the process of turning. Sometimes it is iatrogenic (caused by the provider). If labor is slow, the care provider may break the mother’s waters in an effort to speed up labor. This removes the buoyant cushion that can make it easier for the baby to finish its turn and the baby may end up “stuck” in this position. This is called “Transverse Arrest.” A fair amount of cesareans are caused by transverse arrest.
Compound Presentation
 |
| A nuchal hand presenting alongside the head |
Babies who have their hands up by their faces (a “nuchal hand” or sometimes a nuchal elbow/arm) can present another challenge.
The baby is basically OA and in a great position for birth, but the hand or arm beside the head causes larger-than-average presenting parts that must fit through at the same time. If the care provider can get the baby to pull back its arm/hand near birth, the baby is likely to then be born quickly. If the arm/hand remains by the baby’s head, pushing is likely to be slow, painful, and difficult. Usually babies with nuchal hands can be born vaginally, but there may be quite a bit of tearing and damage to the mother. If the provider is not patient during a slow pushing stage with a nuchal hand/arm, it may result in a cesarean.
Asynclitic Heads
 |
| Asynclitic baby in OA position |
Similarly, babies who have their heads tipped to the side instead of straight (“asynclitic”) also have difficulty fitting. Instead of the top of the head presenting first, their parietal bone (bony side of head) presents first. The tipped head causes a larger than average head diameter that doesn’t fit as easily.
Many asynclitic babies will correct the tilt of their heads if the mother’s waters are kept intact and she is able to be mobile in labor. Asymmetric birth positions may help correct the tilt. Once the tilt is corrected, the baby is often born fairly quickly.
If the baby is not able to correct the tilt of its head on its own, then the care provider may be able to help through the use of a vacuum extractor or forceps. Sometimes the tilt of the head goes undiscovered or is not able to be resolved during labor; these babies often are born by cesarean.
Summary
Unfortunately, many women with a prior cesarean for CPD or Arrest of Descent are discouraged from even trying to have a VBAC. They may be told they have little chance at a VBAC and they should just schedule a planned repeat cesarean rather than risk another cesarean during labor. One woman was told:
You’ve already proven you can’t get a baby out of your pelvis.
Obviously, that OB believed that the pelvis itself was the issue, not the baby’s position, but the recent Arrest of Descent study suggests it is likely not true.
This kind of misleading “guidance” from care providers is not evidence-based. Most women with a prior CPD or Arrest of Descent cesarean who go through with labor actually have a reasonable chance at a VBAC, as this woman found:
The OB that did my c-section told me that my pelvis was small and also tilted and that because of that, a vaginal birth wouldn’t be possible. Well, I…went for a VBAC anyway and it’s a good thing I did because I had a wonderful amazing and natural VBAC with my next baby. And she came out in about 4 pushes. It was so easy! I had my second VBAC with my son a year ago and it went perfectly as well!
Here is a link to the story of another case where a woman who had a cesarean was told that her pelvis was too small to birth a baby and to forget about a VBAC. She went on to birth a 9 lb. baby ─ with a nuchal hand ─ as a VBAC. The Birth Without Fear blog has an awesome picture of it in their birth stories section.
That’s not to say that CPD is never real. Sometimes it is. Although most cases of “CPD” are actually situational (caused by a malposition), sometimes there are rare cases of true CPD. These are usually a result of significant malnourishment in childhood, severe scoliosis, a history of rickets, or a history of a bad fall or accident where the pelvis was damaged. And sometimes, women don’t have any of that in their background, really do try everything, and still end up with a cesarean because the baby just didn’t fit. It does happen and it’s important to acknowledge that.
But far too often, women who have had a cesarean after not being able to push out a baby are told that their pelvises are too small or defective, and they’ll never be able to push out a baby. This is not true. Many women with this history can have a vaginal birth, if given an adequate chance to do so. Anecdotally, many women who have been told this benefit from having a good chiropractor evaluate their back and pelvis to help maximize the space in it and get it well-aligned. See my story below.
Women with a history of cesareans for Arrest of Descent or CPD should be offered the chance at a VBAC if they want it. Chances are good they will have one. There are never any guarantees, but research clearly shows that trying for a VBAC is a very reasonable choice in this group and should not be discouraged.
My Story
Again, many women have had cesareans for arrest of descent and yet gone on to have a VBAC. Conventional wisdom is that you need a smaller baby to get a VBAC, but some women do have VBACs with a baby even bigger than their cesarean baby. Again, fetal position is key.
This includes me. I had my first cesarean after a difficult induced labor. I dilated to 10 cm and pushed for two hours in stirrups, but ended up with a very traumatic cesarean. With my second baby, I had a relatively easy spontaneous labor where I did all the “right” things including position changes but still had FIVE HARD HOURS of pushing with little descent of my deflexed OP baby. I ended up with a second cesarean for CPD.
Both of my babies were big. I was told I had a “marginal” pelvis by my first care provider, and unless I had a smaller baby I would probably not have a vaginal birth. After my second birth, a nurse-midwife told me I probably had a pelvic shape predisposed to posterior babies and my babies would likely always be posterior. After two CPD cesareans at full dilation and after hours of pushing, I was told I was extremely unlikely to have a VBAC. The “VBAC Calculator” gave around a 20% chance of having a VBAC if I tried again.
All these declarations were wrong in the end but it was difficult to have faith. In my third pregnancy, I wavered between choosing to labor again or just going straight to a repeat cesarean. The baby was consistently posterior again all through pregnancy and I had no desire to go through a long hard labor only to end up with another cesarean ─ but neither did I want to go through another surgical recovery. I was also worried about the increase the risk of placental issues from another cesarean if I decided to have another baby in the future.
Near the end of my third pregnancy, I found a chiropractor who did a lot of work on my pelvis, including the Webster Technique and releasing the round ligaments that attach to the uterus. She felt my history of car accidents was highly relevant to the malpositions going on. According to her, the significant back and pubic pain I was having indicated “in utero constraint” that was making it hard for my babies to be in the easiest position for labor. The chiropractic adjustments eased a lot of my discomfort and the baby moved pretty quickly into a more optimal OA position for the first time in three pregnancies!
I went on to have a VBAC after 2 cesareans (VBA2C), something many providers would have told me would be extremely unlikely with my history and risk factors (short, old, “morbidly obese,” big babies, two prior CPD cesareans, no prior vaginal births). Instead of pushing for 2 hours or for 5 hours as I did with my first two children, I pushed for 12minutes with that baby. The doctor didn’t even make it to the birth.
And it wasn’t just a lucky fluke. Several years later, I had another VBA2C, this time with a baby that was a pound larger than either of my cesarean babies. I only pushed for 24 minutes with that baby.
Afterwards I asked my midwife to evaluate my pelvis and tell me honestly if it was truly marginal or not. She examined me and said it absolutely was not. Either the prior evaluation was wrong or chiropractic care really did create more space in my pelvis ─ or maybe a little of both. I do feel that the chiropractic care was integral to my VBACs, given that I never had an anterior baby until I had chiropractic care.
Remember, each labor and birth is unique and previous problems do not necessarily happen again.
Even a history of more than one Arrest of Descent or CPD cesarean does not mean it will continue to happen, especially if the mother is very proactive about fetal position. I had a history of TWO cesareans for Arrest of Descent and still went on to have two VBACs.
I have known women who have had VBACs after 1, 2, and even 3 prior CPD cesareans, including full dilation and pushing for hours each time with no vaginal birth. Yet they still eventually had a VBAC. The International Cesarean Awareness Network (ICAN) has a number of stories of women who have had a prior cesarean (or more) for CPD or Arrest of Descent and yet went on to have a VBAC. You can see some of them in their “Question CPD” video below.
There are never any guarantees, of course, and there are important risks to consider with both VBAC and an Elective Repeat Cesarean. However, if you choose to labor, your VBAC chances are good, anywhere between 50-80% based on the research. Don’t let care providers convince you out of trying for a VBAC based on a past history of CPD or Arrest of Descent. In the end, it’s your decision.
References
J Matern Fetal Neonatal Med. 2018 Feb 27:1-5. doi: 10.1080/14767058.2018.1443069. [Epub ahead of print] Vaginal birth after a cesarean delivery for arrest of descent. Fox NS, Namath AG, Ali M, Naqvi M, Gupta S, Rebarber A. PMID: 29455594
…This was a retrospective cohort study of all patients delivered by a single MFM practice from 2005 to 2017 with a singleton pregnancy and one prior CD for arrest of descent. We estimated the rate and associated risk factors for successful VBAC. RESULTS: We included 208 patients with one prior CD for arrest of descent, 100 (48.1%) of whom attempted a trial of labor after cesarean (TOLAC) with a VBAC success rate [of] 84/100 (84%, 95% CI 76-90%). Among the women who attempted TOLAC, women with a prior vaginal delivery >24 weeks’ had a significantly higher VBAC success rate (91.8% versus 71.8%, p = .01). Maternal age, body mass index, estimated fetal weight, induction of labor, and cervical dilation were not associated with a higher VBAC success rate. CONCLUSIONS: For women with a prior CD for arrest of descent, VBAC success rates are high. This suggests that arrest of descent is mostly dependent on factors unique to each pregnancy and not due to an inadequate pelvis or recurring conditions. Women with a prior CD for arrest of descent should not be discouraged from attempting TOLAC in a subsequent pregnancy due to concerns about the likelihood of success.
J Matern Fetal Neonatal Med. 2017 Feb;30(4):461-465. Epub 2016 May 5. Prolonged second stage in nulliparous with epidurals: a systematic review.Gimovsky AC, Guarente J, Berghella V. PMID: 27050812
…A systematic review of the literature was performed… for case series evaluating the morbidities of prolonged second stage of labor. Search terms used were “prolonged”, “second stage”, and “labor”. Prolonged second stage was defined as three hours or more. Retrospective case series of prolonged second stage in nulliparous women with epidurals were identified. The primary outcome was the incidence of cesarean delivery. RESULTS: Two retrospective series with 5350 nulliparous women with prolonged second stage were identified. 76.3% (4 081/5 350) had an epidural. Of all nulliparous women with an epidural, 11.5% (4 081/35 469) had prolonged second stage. Cesarean Delivery occurred in 19.8% of these cases (782/4 081), while 80.2% had a vaginal delivery. CONCLUSIONS: Over three quarters of nulliparous women with epidural diagnosed with a prolonged second stage deliver vaginally.
“…Even with a history of CPD, two-thirds of women will have successful VBAC, though rates decrease with increasing numbers of prior CS…There are few absolute contraindications to attempted VBAC. Attempted VBAC will be successful in the majority of attempted cases.”
Obstetrics and Gynecology. February 1989. 73(2):161-5. Twice A Cesarean, Always a Cesarean? Phelan, JP et al. PMID: 2911420
[My summary of highlights from the full text] 501 women with 2 or more previous cesareans had a TOL, and 69% had a VBAC overall. Women who had had at least one previous cesarean for CPD had a 64% VBAC rate. Those who had had 2 successive labors both ending in c/s for CPD still had a 56% VBAC rate. In other words, even those women with a previous ‘failed’ trial of labor had a better chance of a VBAC than another cesarean in labor.
Other Studies on Arrest of Descent or Similar Definitions
-
Am J Obstet Gynecol. 2015 Dec;213(6):861.e1-5. doi: 10.1016/j.ajog.2015.08.064. Epub 2015 Sep 6. Effect of stage of initial labor dystocia on vaginal birth after cesarean success. Lewkowitz AK, Nakagawa S, Thiet MP, Rosenstein MG. PMID: 26348381
- Acta Obstet Gynecol Scand. 2013 Feb;92(2):193-7. doi: 10.1111/aogs.12023. Epub 2012 Nov 5. Cervical dilation at the time of cesarean section for dystocia — effect on subsequent trial of labor.Abildgaard H, Ingerslev MD, Nickelsen C, Secher NJ. PMID: 23025257
- Obstet Gynecol. 2001 Oct;98(4):652-5. Should we allow a trial of labor after a previous cesarean for dystocia in the second stage of labor?Bujold E, Gauthier RJ. PMID: 11576583
- Obstet Gynecol. 2000 Apr;95(4): S38. https://doi.org/10.1016/S0029-7844(00)00660-8 Obstetrics Prognostic indicators for successful vaginal birth after cesarean delivery. Marshak J, Cooperman BS, Fried WB, Shi, Quihu. Available here.
- Br J Obstet Gynaecol. 1998 Oct;105(10):1079-81. Vaginal delivery after previous caesarean section for failure of second stage of labour. Jongen VH, Halfwerk MG, Brouwer WK. PMID: 9800930
- Obstet Gynecol. 1998 Nov;92(5):799-803. First delivery after cesarean delivery for strictly defined cephalopelvic disproportion. Impey L, O’Herlihy C. PMID: 9794672
- Obstet Gynecol. 1997 Apr;89(4):591-3. Correlation between maximum cervical dilatation at cesarean delivery and subsequent vaginal birth after cesarean delivery. Hoskins IA, Gomez JL. PMID: 9083318
Blog reposted with permission of Pamela Vireday. You can check out her original post here.